When Martina began to lose her vision, she thought it was simply part of aging.
As a grandmother to five, she spent her time taking care of her grandchildren, allowing her daughter to work and support her family. When her sight began to cloud, Martina began leaning on her daughter for guidance.
Within a couple years, Martina was blind from cataracts—a condition curable with a 20-minute surgical procedure. Her daughter left her job to care for Martina. Her grandchildren no longer received the care they had previously received. What began as one woman’s vision loss became an entire family’s economic crisis.
Then Martina attended an Eye Corps outreach camp. The morning after her surgery, Martina removed her patch and saw her daughter and grandchildren for the first time in years. Within weeks, her daughter returned to work, and Martina returned to primary caregiver for her grandchildren. Yet, the impact of the surgery didn’t end there. With restored vision and health, Martina opened a small shop in her house to help support her family.
Sight restored. Dignity restored. Opportunity restored. A single surgery transformed the future of three generations. And it all started with a donor’s dollar.
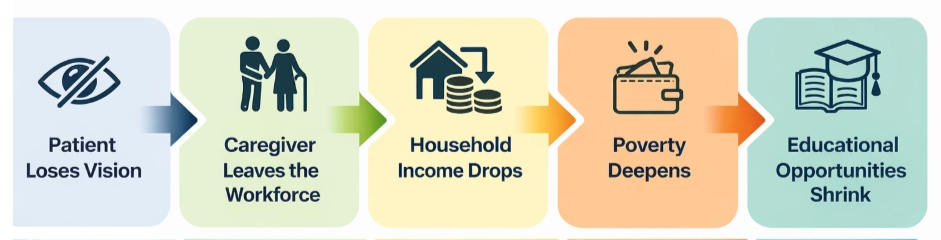
While Martina’s story is deeply moving, her story is not uncommon. In Tanzania, an estimated 8.2 million people live with vision loss, predominantly affecting women and young girls. The country has fewer than 80 ophthalmologists serving over 67 million people—approximately one ophthalmologist for every 837,500 Tanzanians. The country is severely underserved, with nearly half of Tanzanians living in extreme poverty and nearly 12% living with vision loss—two factors that reinforce one another in a devastating cycle:
Blindness in Tanzania is not often the result of a complex disease. Here’s the good thing—in many cases, it's caused by cataracts or uncorrected refractive errors, both of which are very treatable conditions. The tragedy is not medical complexity: it is lack of access to care.
Tanzania’s state of crude vision loss is nearly double that of neighboring East African states, largely due to a shortage of skilled ophthalmologists and accessible, affordable care. Restoring sight has been shown to significantly increase family earning potential by returning both the patient and their caregiver to the workforce. In other words, vision care is not simply healthcare. It is economic development.
Consider the economics of a single cataract surgery. When a donor funds surgery for one patient, the impact ripples outward:
Multiply that effect across the 19,366 patients treated in 2024 alone. Now extend it across the next decade.
Eye Corps’ long-term scaling plan projects treatment of more than 1.2 million additional patients, while driving cost efficiency to approximately $60 per patient as infrastructure expands. That is not simply charitable reach. It is systems thinking at scale.
For philanthropic leaders thinking in generational terms, this distinction matters. Sustainable health interventions do more than solve an immediate problem — they strengthen local capacity, expand leadership, and unlock long-term economic mobility.
The long-term solution to blindness in Tanzania is not short-term intervention. It is workforce development. After residency training at Eye Corps facilities, young ophthalmologists receive mentorship, surgical instruments, and outreach coordination as they establish practices in underserved regions. By year five, these physicians achieve practice self-sustainability, gaining an invaluable entrepreneurial skillset. At that point, philanthropic dollars shift primarily toward outreach camps serving the poorest patients.
The result is a virtuous cycle:
.png)
When thinking about the impact of your dollar, it is important to remember that this is not a temporary mission-based model. Eye Corps promotes an ecosystem designed for longevity. So who is the most affected by the prevalence of blindness in Tanzania? Women. Women represent 64% of the world’s blind population and are significantly less likely to receive cataract surgery. In Tanzania, barriers to care for women include transportation challenges, financial constraints, cultural bias, and family dynamics. Over the past several years, there has been measurable progress: women represented 35% of patients treated in 2021, increasing to 47% in 2024.
When a grandmother regains sight, she resumes childcare and household leadership. When a mother regains sight, children stay in school and income stabilizes. The economic return on restoring women’s vision extends well beyond the individual. The ripple effects are profound.
So why Tanzania and why now? The answer is simple: it’s solvable. Tanzania’s blindness crisis is driven by a simple imbalance with high need, high poverty, and low provider density. With fewer than 80 ophthalmologists nationwide, the opportunity for leverage is extraordinary. Training one ophthalmologist today means thousands of surgeries over a career, tens of thousands of lives impacted, and a generation of future surgeons mentored. By 2034, Eye Corps plans to graduate and train 212 ophthalmologists, treat 1.26 million patients, and expand outreach to 20 regions across the country. The scale of transformation is measurable. But the human impact remains deeply personal.
For centuries, blindness has been associated with dependency and marginalization. Yet today, much of global blindness is preventable. The barrier is no longer medical knowledge — it is equitable distribution of training, equipment, and infrastructure.
When a donor funds cataract surgery in Tanzania, they are not simply restoring sight. They are:
They are investing not only in vision — but in economic resilience.
Martina’s restored sight did more than allow her to see her grandchildren again. It allowed her daughter to return to work. It allowed her grandchildren to remain in school. It allowed her to open a small shop and contribute to her household’s income. Access to a simple surgery transformed three generations.
That is the impact of a donor’s dollar.
